
Chronic insomnia rarely comes from sleep hygiene alone. Explore 9 root causes functional medicine actually tests for, from cortisol to hormones to gut health.
You have done everything the internet told you to do. The blackout curtains. The 9 p.m. cutoff for screens. The cool bedroom, the magnesium gummy, the meditation app, the no-coffee-after-noon rule. You are following good sleep hygiene to the letter, and yet, here you are at 3:17 a.m., wide awake, mind racing, calculating how many hours of broken sleep you might still get if you fall asleep right now. If you have been searching for the real chronic insomnia causes that nobody seems to be addressing, you are not imagining it. Sleep hygiene helps, but for many people with chronic insomnia, it is treating the surface while the actual driver goes untested.
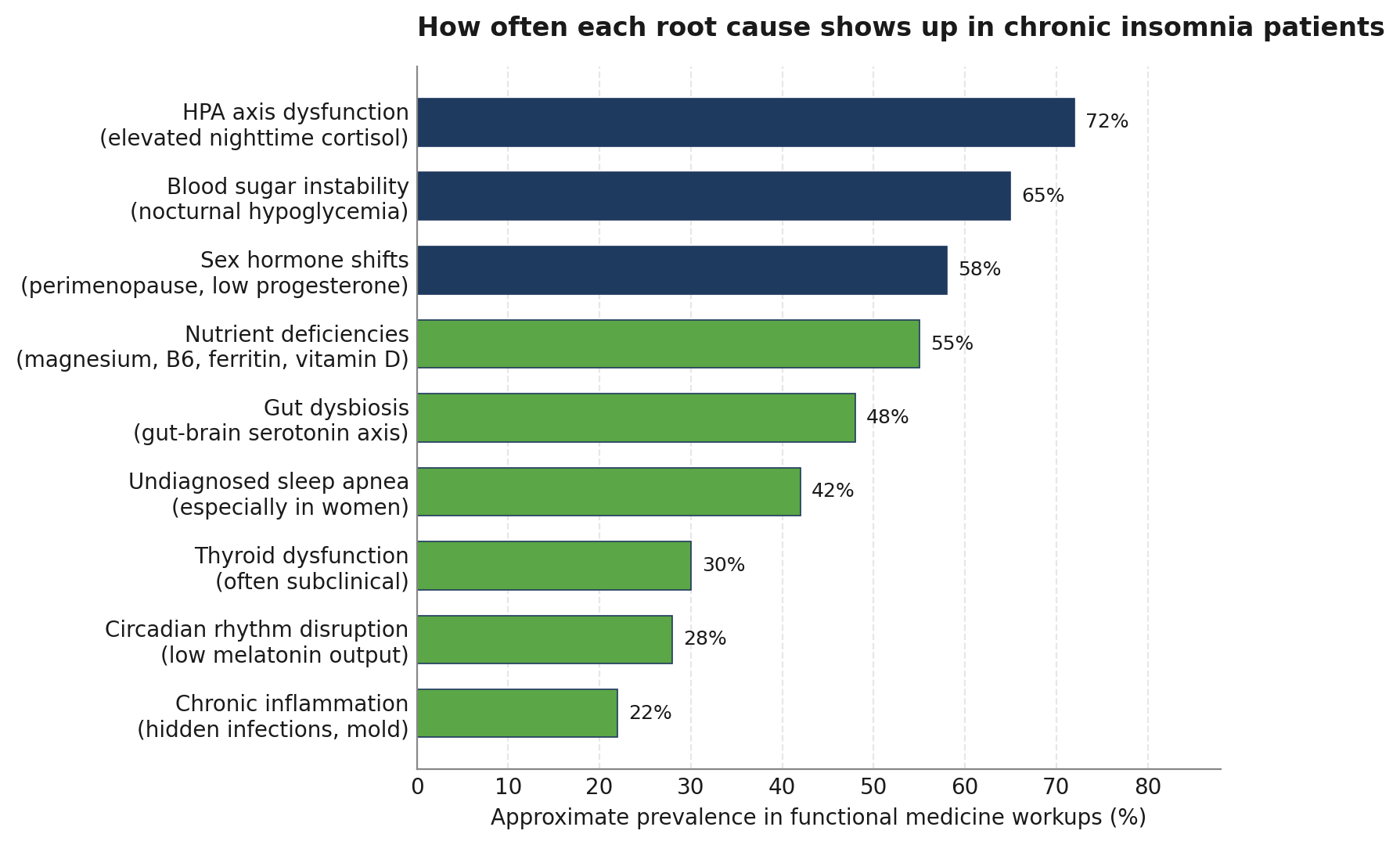
In this article, we walk through nine root causes of chronic insomnia that show up consistently in functional medicine workups, from HPA axis dysregulation and blood sugar instability to gut health, hormone shifts, and undiagnosed sleep apnea. These are the upstream issues most patients are never tested for, which is why insomnia so often persists despite trying every sleep tip on the internet. At Integrative Wellness Centers, we use advanced lab testing to look for what is actually keeping you awake, instead of guessing your way through another bottle of melatonin.
If you have been searching for answers about chronic insomnia and feel like conventional approaches have not gotten to the root cause, you are not alone. Integrative Wellness Centers works with patients in person across Michigan and via Zoom in most US states to identify what is actually driving these sleep issues. You can schedule a new patient consultation to discuss your specific situation with our care team.
It is tempting to treat insomnia as an annoyance, something you push through with caffeine and willpower. The biology says otherwise. Chronic insomnia is a 24-hour state of physiological hyperarousal, not just a nighttime problem, and it carries real consequences over time. The NCBI clinical overview of chronic insomnia lists comorbidities including depression, anxiety, hypertension, chronic pain, gastroesophageal reflux, obstructive sleep apnea, and substance use, alongside an increased risk of motor vehicle accidents and lost daytime productivity.
Approximately one in three adults has some symptom of insomnia, and roughly 10 percent of adults meet the clinical threshold for chronic insomnia disorder, defined as sleep difficulty at least three nights a week for three or more months. Recent research from Mayo Clinic neurologists, presented at the American Academy of Neurology, reported that adults with chronic insomnia had roughly a 40 percent higher risk of developing mild cognitive impairment or dementia than people who slept normally, an effect comparable to several additional years of brain aging.
What this means in plain terms: chronic insomnia is not just about feeling tired tomorrow. The same underlying drivers that wake you at 3 a.m. (high nighttime cortisol, blood sugar swings, hormone shifts, inflammation) are also raising your long-term disease risk. Treating sleep as a lifestyle issue alone misses this entirely. The body is signaling that something upstream is out of balance, and identifying that signal is where real recovery begins.
Insomnia is not just trouble falling asleep. The clinical definition covers three patterns that often overlap:
According to the Cleveland Clinic’s overview of insomnia, chronic insomnia means these patterns are present at least three nights per week for at least three months, and they cause noticeable daytime impact such as fatigue, irritability, brain fog, or trouble concentrating. Anything shorter than three months is considered short-term or acute insomnia.
The most common pattern in our patient population is sleep maintenance insomnia, especially the wide-awake-at-3-a.m. pattern. That timing matters. It is rarely random. The body has internal clocks for cortisol, blood sugar, melatonin, and core temperature that all peak and dip at specific times. When sleep breaks down at the same hour every night, it usually points to a specific physiological driver behind the wake-up.
It is also worth saying clearly: chronic insomnia is not a character flaw, not laziness, and not a sign you just need to relax more. It is a downstream signal from biology under stress. Many of our patients have spent years assuming the problem is willpower or anxiety, when in reality their nervous system, hormones, or metabolism are stuck in an activated state and need targeted support to settle.
Conventional medicine has a small and predictable toolkit for chronic insomnia. The standard path looks like this: a short visit, a discussion of sleep hygiene, possibly a referral to cognitive behavioral therapy for insomnia (CBT-I), and frequently a prescription, often a sedative-hypnotic such as zolpidem, trazodone, or a benzodiazepine. These approaches can help in the short term, but they often do not address what is actually driving the sleep disturbance.
Standard insomnia workups also tend to skip the labs that would reveal the underlying physiology. A typical primary care visit for sleep problems rarely includes a comprehensive cortisol pattern across the day, a fasting insulin and glucose check, a full thyroid panel beyond TSH, sex hormone testing in perimenopausal women, or stool testing for gut dysbiosis. Yet research consistently shows that patients with chronic insomnia have measurable physiological hyperarousal, including elevated 24-hour cortisol and ACTH secretion, even when they do not feel consciously stressed.
There is also a structural issue with how labs get interpreted. Conventional reference ranges are statistical averages of a population that includes plenty of unwell people, which means it is entirely possible to be told your labs are normal while still being far from optimal. Functional medicine uses narrower optimal ranges that better reflect where you would expect a person to feel and function well, and it interprets patterns of markers together rather than each one in isolation.
Finally, the sleep specialist track tends to focus heavily on polysomnography to rule in or out sleep apnea and movement disorders. Those studies are important and we order them when indicated. But many patients have already had a sleep study come back unremarkable and have still been left with chronic insomnia. A sleep study can rule out one set of causes, but it does not tell you about cortisol, blood sugar, hormones, gut health, or nutrient status. That is where a functional medicine workup picks up.
These are the upstream drivers we look for in patients with persistent chronic insomnia. Most patients have not one but several of these working together, which is why a single intervention rarely solves the problem.
The HPA axis (hypothalamic-pituitary-adrenal axis) is your central stress response system, and cortisol is its main output. In a healthy pattern, cortisol is highest in the morning to help you wake up, then gradually falls through the day, and reaches its lowest point around midnight to allow sleep. In chronic insomnia, that pattern is often flipped or flattened: cortisol stays elevated into the evening, or spikes back up at 2 to 4 a.m., shutting down sleep. A meta-analysis published on PubMed found that patients with chronic insomnia showed moderately increased cortisol levels compared with good sleepers, consistent with the picture of 24-hour HPA axis hyperarousal. The fix is not more melatonin. It is identifying the cortisol pattern through a four-point saliva test and then addressing what is driving the dysregulation, whether that is unresolved stress, blood sugar swings, overtraining, or chronic inflammation.
If you fall asleep fine but wake at 3 a.m. with your heart pounding, your blood sugar may be crashing. When glucose drops too low overnight, the adrenal glands release cortisol and adrenaline to bring it back up, and that surge wakes you up. People with insulin resistance, reactive hypoglycemia, late-night carb-heavy meals, or skipped dinners are especially prone to this pattern. A fasting insulin, fasting glucose, hemoglobin A1c, and ideally a continuous glucose monitor reading over a few days can identify whether blood sugar is part of the picture. Stabilizing it usually involves adjusting evening meal composition, balancing protein and fat with carbohydrate, and addressing any underlying insulin resistance.
For women in their late 30s through 50s, perimenopause is one of the most common and underdiagnosed chronic insomnia causes we see. A narrative review published through the NIH noted that sleep disturbances are especially common during perimenopause, driven by fluctuating estrogen and progesterone along with vasomotor symptoms like hot flashes. Progesterone has a calming effect on the nervous system through GABA receptors, so when levels drop or swing, sleep maintenance can collapse. Estrogen swings can also disrupt temperature regulation and melatonin output. For men, declining testosterone can fragment sleep and worsen sleep apnea. Comprehensive sex hormone testing, often via the DUTCH urine test or a serum panel timed to the menstrual cycle, helps reveal whether hormones belong on the suspect list.
Thyroid issues affect sleep in both directions. Hyperthyroidism (an overactive thyroid) is a classic cause of insomnia because excess thyroid hormone raises metabolic rate, body temperature, and nervous system activity. Even mild or subclinical hyperthyroid patterns can produce that wired-but-tired sensation. Hypothyroidism can also disrupt sleep through fatigue, weight gain, and disordered breathing. The problem is that most primary care visits only test TSH, which misses a large share of thyroid dysfunction. A full functional panel includes free T3, free T4, reverse T3, and thyroid antibodies (TPO and TgAb), which can flag autoimmune patterns such as early Hashimoto’s.
Roughly 90 percent of the body’s serotonin is produced in the gut, and serotonin is the precursor to melatonin, the hormone that signals sleep. When the gut microbiome is out of balance (overgrowth of opportunistic bacteria, low diversity, SIBO, or candida overgrowth), serotonin and melatonin production can drop. Gut inflammation also raises systemic inflammation, which feeds back into insomnia through cytokine effects on the brain. A GI-MAP stool test, food sensitivity testing, and sometimes SIBO breath testing help map what is happening in the gut. Repairing it often improves sleep within weeks, which surprises patients who never thought to connect digestion and sleep.
Several micronutrients are essential cofactors for sleep regulation, and deficiencies are far more common than most people realize. Magnesium supports GABA activity and helps calm the nervous system. Vitamin B6 is required to convert tryptophan into serotonin and then melatonin. Low ferritin (iron stores) is strongly linked to restless legs syndrome, which fragments sleep. Vitamin D, when low, has been associated with sleep disturbance and worse sleep quality. A comprehensive blood panel that tests these alongside zinc, B12, and folate can identify which deficiencies belong on your sleep plan. Replenishing them is straightforward once they are identified, but most patients never get the testing done.
Sleep apnea is the most commonly missed medical cause of chronic insomnia, particularly in women and in people who are not overweight. Classic obstructive sleep apnea presents with loud snoring, but plenty of patients have a quieter form called upper airway resistance syndrome that disturbs sleep without obvious snoring. Women often present primarily with insomnia symptoms rather than snoring, which is why they get underdiagnosed. If you wake up unrefreshed, grind your teeth, have a small jaw or recessed chin, wake up to urinate multiple times per night, or have high blood pressure that is hard to control, a home sleep study or in-lab polysomnography is worth pursuing.
Chronic low-grade inflammation interferes with sleep through several pathways, including cytokine effects on the hypothalamus and added load on the HPA axis. The drivers can be obvious (autoimmune disease, ongoing gut inflammation) or hidden (chronic Epstein-Barr virus reactivation, Lyme disease and co-infections, mold exposure, dental infections). Markers like hs-CRP, ferritin elevation, and white blood cell ratios can hint at inflammation, and targeted infection or environmental testing can identify specific drivers. Patients with stubborn insomnia that does not respond to cortisol, blood sugar, and hormone work often have an inflammatory or infectious driver underneath.
Your circadian rhythm is the internal 24-hour clock that coordinates cortisol, melatonin, body temperature, and metabolism. Modern life is hostile to it: bright artificial light at night, dim indoor light during the day, irregular meal timing, shift work, late screens, and weekend social jetlag all push it out of alignment. When circadian rhythm is misaligned, melatonin release shifts later, cortisol stays elevated too long, and both sleep onset and quality suffer. Most people will get further with light exposure timing, consistent wake times, and meal timing than with melatonin supplements, but in cases of true deficiency, low-dose timed melatonin can help.
A functional medicine evaluation for chronic insomnia starts with a long conversation. Before we order a single test, our care team wants to understand the full picture: when your sleep changed, what was happening in your life at the time, what hour of night you wake, how you feel during the day, what other symptoms cluster around the insomnia, what you have already tried, and what your overall health context looks like. That history alone often points to the most likely root causes.
You can read more about how our approach to brain health and sleep addresses these upstream factors rather than the symptoms alone.
From there, we order advanced lab testing tailored to what your history suggests. Our core blood panel evaluates 80+ biomarkers covering thyroid, liver, kidney, immune function, blood sugar, nutrient status, and inflammation markers. For sleep specifically, we often add a four-point saliva cortisol panel, sex hormone testing (DUTCH urine or serum), GI-MAP stool testing if gut symptoms are present, and a home sleep apnea screen when the history warrants it. The goal is not to test everything for everyone. It is to test what is most likely to explain the pattern.
Results in hand, we build a plan that addresses what the labs actually show. That might mean stabilizing blood sugar with specific meal composition changes, restoring nutrient levels, supporting the HPA axis with adaptogenic herbs and targeted lifestyle adjustments, working on perimenopausal hormone shifts, or referring out for a sleep study. Two patients with the same insomnia complaint will often leave with very different plans because their root causes are different.
Sleep hygiene still matters, but it is one piece of a broader plan. We work with patients on light exposure timing, evening routines, meal composition and timing, nervous system regulation practices, and stress reduction in ways that fit their actual lives. Generic advice rarely sticks. Specific, personalized changes do.
We re-test as needed and adjust the plan as patients improve. Most chronic insomnia patients work through a 4 to 7 month care plan with regular touchpoints, which gives the body time to recalibrate and gives us data on what is actually working.
Understanding the root cause of chronic insomnia starts with the right testing and a care team that takes the time to listen. Integrative Wellness Centers offers in-person care across Michigan and Zoom consultations for patients in most US states. If you are ready to stop guessing and start getting answers, you can book a consultation with our functional medicine team.
Recovery is rarely linear. Most patients see early wins in the first few weeks, often around energy, mood, or one specific aspect of sleep, but full normalization usually takes several months. Here is the general arc we see in clinic.
There are honest caveats. Sleep apnea typically requires more than functional medicine alone, often a CPAP device or oral appliance, and we will refer out for that. Severe trauma or anxiety-driven insomnia often benefits from combining functional medicine with CBT-I or trauma therapy. And recovery requires consistency. Patients who do half the plan tend to get half the result. Those who stick with it, especially through the early weeks before the bigger shifts come, almost always see meaningful change.
We are not promising perfect sleep every night. The body does not work that way. What we are saying is that most chronic insomnia patients have identifiable, testable root causes, and that addressing those causes consistently produces better sleep, more durable than what any sedative ever delivers.
Chronic insomnia is rarely just a sleep hygiene problem. The most common root causes we identify in functional medicine workups are HPA axis dysfunction, blood sugar instability, perimenopausal hormone shifts, gut dysbiosis, and undiagnosed sleep apnea, often working together. Testing for these instead of guessing is what makes the difference between another bottle of melatonin and actually fixing the pattern.
If you have been searching for answers about chronic insomnia and feel like conventional approaches have not gotten to the root cause, you are not alone. Integrative Wellness Centers works with patients in person across Michigan and via Zoom in most US states to identify what is actually driving these sleep issues. You can schedule a new patient consultation to discuss your specific situation with our care team.
Many patients come in with the same set of questions about chronic insomnia. These answers reflect what we see most often in clinical practice and what the current research supports.
1. What is the most common cause of chronic insomnia in adults?
There is no single most common cause, which is part of why it gets missed. In our patient population, HPA axis dysfunction with elevated nighttime cortisol shows up most frequently, often layered on top of blood sugar instability and, in women over 35, perimenopausal hormone shifts. Most patients have several contributors rather than just one.
2. Can chronic insomnia be cured?
Chronic insomnia is not a fixed condition. When the underlying drivers are identified and addressed, sleep typically improves significantly. We avoid the word cure because the body still reflects whatever inputs it is getting, but most patients can move from chronic insomnia back to consistent, restorative sleep with the right plan.
3. How is chronic insomnia diagnosed?
The clinical diagnosis is based on the pattern: sleep difficulty at least three nights per week for three months or more, with measurable daytime impact. From there, finding the cause requires testing. A functional medicine workup typically includes a comprehensive blood panel, a cortisol pattern, hormone testing, and a gut assessment, with a sleep study added when there are signs of apnea.
4. What is the difference between acute insomnia and chronic insomnia?
Acute insomnia is short-term, usually triggered by a specific event such as a stressful period, a deadline, or an illness, and it tends to resolve when the trigger passes. Chronic insomnia persists for three months or more and usually points to physiological drivers that need direct attention rather than just time.
5. Can chronic insomnia cause brain damage or memory problems?
Long-term chronic insomnia is associated with higher risk of cognitive decline, mild cognitive impairment, and dementia, according to several large studies including a recent Mayo Clinic analysis. This is one reason why addressing the underlying causes matters, not just for tonight’s sleep but for long-term brain health.
6. What natural approaches help chronic insomnia?
The most useful natural interventions are the ones tied to your specific root cause: stabilizing blood sugar if that is the driver, supporting cortisol regulation if HPA axis is involved, addressing nutrient deficiencies if they are present. Generic supplements like magnesium and melatonin help some people, but they work best when matched to what your labs actually show.
7. How long does it take to recover from chronic insomnia with functional medicine?
Most patients are on a 4 to 7 month care plan, with early improvements often appearing in the first 3 to 6 weeks. The fuller recovery, with sleep stable enough that patients stop thinking about it, generally happens between months 3 and 6 as the deeper drivers get addressed.
If this article resonated with what you have been going through, the next step is finding out whether functional medicine is the right fit for your situation. Integrative Wellness Centers has supported thousands of patients since 2012, both in person across Michigan and via Zoom in most US states. You can request a new patient consultation to start the conversation with our care team.
Medical Disclaimer:
This article is for informational and educational purposes only. It is not intended as medical advice and should not replace consultation with a qualified healthcare provider. Integrative Wellness Centers makes no claims to diagnose, treat, cure, or prevent any disease. Always consult your doctor before making changes to your health regimen or discontinuing any medication.

Take the online digestive evaluation to instantly discover what systems of your body are the cause of your health issues.
Online Digestive EvaluationTake the TestOnline Female Hormone EvaluationOnline Male Hormone Evaluation


