
Vertigo causes go beyond BPPV and inner ear crystals. Discover the 8 root causes functional medicine investigates, from hormones to nutrients to stress and gut health.
The room starts to spin, your stomach turns, and you have to grab the wall just to stay upright. Maybe it happens when you roll over in bed, when you stand up too fast, or for what feels like no reason at all. You see your primary care doctor, maybe an ENT, possibly a neurologist. They run a few tests, perform the Epley maneuver, hand you a prescription for meclizine, and tell you to come back if it gets worse. But for many people, that is exactly what happens. The episodes keep coming back, the fatigue lingers between them, and no one seems to be asking why vertigo keeps happening in the first place.
Understanding vertigo causes is more nuanced than the standard explanation of "crystals in your ears." Vertigo is a symptom, not a diagnosis, and the conditions that trigger it can range from inner ear disorders to hormonal shifts, nutrient deficiencies, chronic stress, and gut dysfunction. This article walks through the eight root causes of vertigo a functional medicine workup investigates, including the ones conventional medicine often misses. The goal is to give you a clearer map of what could be driving your symptoms so you can pursue answers that go beyond temporary relief. At Integrative Wellness Centers, our team has helped patients track vertigo back to causes their previous doctors never tested for.
If you have been searching for answers about vertigo causes and feel like conventional approaches have not gotten to the root of the problem, you are not alone. Integrative Wellness Centers works with patients in-person across Michigan and via Zoom in most US states to identify what is actually driving recurrent dizziness and spinning episodes. You can schedule a new patient consultation to discuss your specific situation with our care team.
Vertigo affects an estimated 15 to 20 percent of adults each year, and roughly 30 percent of people will experience a significant episode at some point in their life. It is one of the most common reasons people end up in emergency rooms and primary care offices. Most cases are not life-threatening, but the impact on daily life can be severe. People stop driving. They miss work. They cancel social plans because they cannot predict when the next attack will come. Falls become a real concern, especially for adults over 60, where vertigo-related falls are a leading cause of hip fractures.
The frustrating reality is that vertigo often goes underexplored. The standard workup focuses on ruling out the most serious causes (stroke, tumor, vascular issues) and identifying the most common one, BPPV. Once those are addressed, many patients are sent home with medications that suppress symptoms without identifying why the vestibular system became unstable in the first place. For people whose vertigo keeps coming back, that approach can feel like running in circles. Knowing the full range of possible vertigo causes gives you and your care team a much better starting point.
Vertigo is the false sensation that you or your surroundings are moving or spinning. It is not the same as general dizziness, lightheadedness, or feeling faint, though many people use these terms interchangeably. According to Cleveland Clinic's overview of vertigo, the most common form is peripheral vertigo, which originates in the inner ear or the vestibular nerve. The less common but more serious form is central vertigo, which involves the brain itself, including conditions like stroke, multiple sclerosis, or vestibular migraine.
Common vertigo symptoms include:
Episodes can last seconds, minutes, hours, or in some cases, days. The duration and triggers often give important clues about the underlying cause. BPPV episodes are usually brief and triggered by specific head positions. Vestibular migraine episodes can last hours and may or may not include headache. Meniere's disease episodes are often longer and accompanied by hearing changes. Identifying the pattern is the first step toward identifying the cause.
When you walk into a conventional medical appointment with vertigo, the standard protocol is straightforward. The doctor screens for red flags like stroke and brain injury, performs a Dix-Hallpike test to check for BPPV, and may prescribe medication to suppress symptoms. If BPPV is confirmed, the Epley maneuver is often performed. If it is not, the explanation often becomes "it is just inner ear issues, give it time." A peer-reviewed review on vestibular disorders and hormonal dysregulation published in PMC notes that despite the prevalence of vertigo, very few studies have looked at hormonal contributors or other systemic root causes, leaving a significant gap in care.
There are a few reasons this gap exists. Insurance-driven appointments tend to be short, often under 15 minutes, which leaves little time to explore patterns beyond the most obvious cause. Standard blood work focuses on medical ranges, which are designed to catch frank disease, not the subtle imbalances in nutrients, hormones, or blood sugar that can affect the vestibular system long before disease develops. And the way medical specialties are siloed means an ENT may not look at your thyroid panel, an endocrinologist may not consider how cortisol affects inner ear fluid, and a neurologist may not investigate the gut as a source of inflammation. Each specialist sees a piece of the picture. Functional medicine is built to look at the whole picture.
Here is a side-by-side comparison of how conventional and functional medicine approach the same patient presenting with recurrent vertigo:
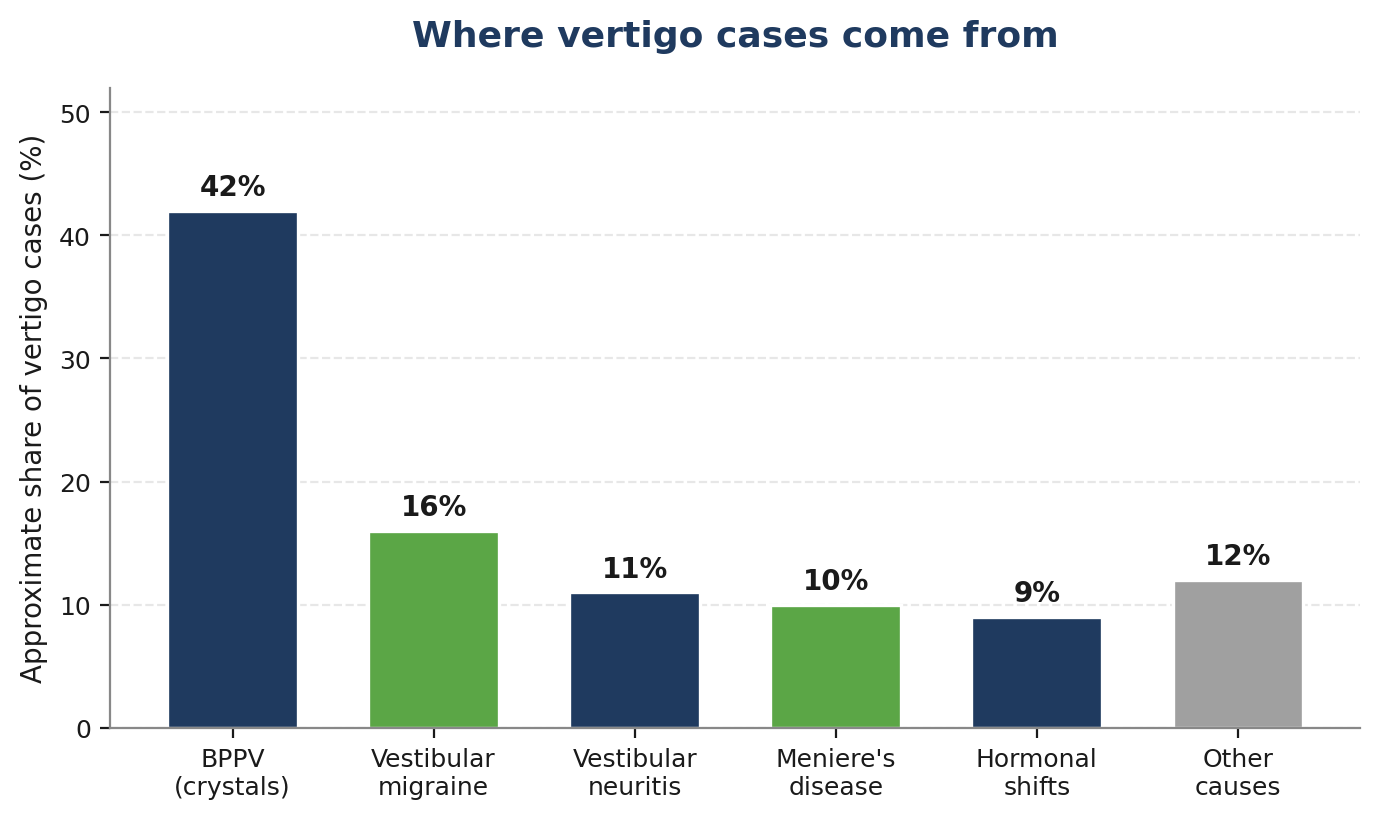
Vertigo is rarely caused by one isolated issue. Often, several factors stack on top of each other. A patient with BPPV may also have low vitamin D, perimenopausal hormone shifts, and chronic stress, all of which make the vestibular system more vulnerable to dysfunction. Here are the eight root causes a thorough vertigo workup investigates.
BPPV is the most common cause of vertigo and accounts for nearly half of all peripheral vertigo cases. It happens when tiny calcium carbonate crystals (otoconia) become dislodged from their normal location in the utricle and drift into the semicircular canals of the inner ear. When you move your head, those misplaced crystals send false signals to your brain, triggering brief but intense spinning sensations. Episodes typically last under a minute and are reliably triggered by lying down, rolling over, or tilting the head back.
The Epley maneuver successfully resolves BPPV for most patients on the first attempt. But here is what often gets missed. BPPV recurs in roughly half of patients within a year, and recurrence has been strongly linked to vitamin D deficiency. A meta-analysis published on PubMed Central looking at vitamin D and BPPV found that patients with recurrent BPPV consistently had lower vitamin D levels than controls, and that supplementation reduced annual recurrence rates. If you have had BPPV more than once, your vitamin D status is worth investigating regardless of what your last lab said.
Vestibular migraine is one of the most underdiagnosed causes of vertigo, especially in women. It is the second most common cause of recurrent vertigo after BPPV and may account for as many as 1 in 7 cases. Unlike classic migraine, vestibular migraine episodes do not always include a headache. The spinning, motion sensitivity, and visual disturbances can show up on their own, which is why so many patients are told their symptoms are "anxiety" or "stress" before the actual diagnosis is made.
Common triggers include stress, poor sleep, hormonal fluctuations, certain foods (aged cheese, alcohol, processed meats, MSG), bright lights, and weather changes. From a functional medicine perspective, vestibular migraine is often a signal that the nervous system has become hypersensitive. The work focuses on identifying triggers, lowering inflammation, supporting mitochondrial function, and addressing magnesium, riboflavin, and CoQ10 status, all of which have evidence supporting their role in migraine prevention.
Meniere's disease is a chronic inner ear disorder characterized by episodes of vertigo lasting 20 minutes to several hours, fluctuating hearing loss, tinnitus, and a feeling of fullness in the affected ear. The underlying mechanism involves abnormal fluid buildup (endolymphatic hydrops) in the inner ear. Conventional treatment usually involves low-sodium diets, diuretics, and sometimes injections or surgery for severe cases.
What conventional treatment often does not address is why fluid regulation in the inner ear went wrong in the first place. Functional medicine investigates contributors like food sensitivities (gluten and dairy are common triggers), chronic viral infections, autoimmune reactivity, and stress-driven changes in fluid balance. Sodium restriction is a useful starting point, but for many patients, the deeper drivers sit upstream of salt intake.
Vestibular neuritis is inflammation of the vestibular nerve, usually triggered by a viral infection. Labyrinthitis is a closely related condition that also involves hearing loss because the cochlear branch of the nerve is affected. Both can cause severe, continuous vertigo that lasts days to weeks, often accompanied by nausea and significant balance problems. Most people recover within a few weeks, but a substantial minority go on to develop persistent dizziness that lingers for months or longer.
When vertigo persists long after the initial infection has cleared, functional medicine looks at immune function, chronic viral reactivation (Epstein-Barr, herpes family viruses, Lyme co-infections), and inflammation. The goal is to support the body's ability to fully resolve the original inflammatory event rather than letting it become a low-grade, ongoing process that keeps the vestibular system unstable.
Hormones have a profound effect on the vestibular system, and this is one of the most overlooked contributors to vertigo in women. Estrogen has modulating effects on the inner ear and on serotonin pathways involved in vestibular function. During perimenopause, estrogen levels swing erratically, and many women develop vertigo, dizziness, or vestibular migraine for the first time during this transition. Research has documented a clear link between vestibular migraine and the perimenopausal period in studies indexed on PubMed, though the connection is rarely raised in standard ENT or primary care visits.
Thyroid dysfunction is another hormonal driver. Both hypothyroidism and hyperthyroidism have been linked to balance disturbances and increased BPPV risk. The catch is that conventional thyroid testing usually checks only TSH, which can miss patients whose Free T3, Free T4, Reverse T3, or thyroid antibodies are out of optimal range. A comprehensive thyroid panel often reveals problems standard testing would not catch.
Nutrient status has a much bigger impact on vestibular function than most people realize. Vitamin D deficiency is consistently associated with BPPV occurrence and recurrence, and supplementation has been shown to reduce attacks in deficient patients. Low vitamin B12 can cause neurological symptoms including dizziness, balance issues, and tingling. Iron deficiency, common in menstruating women and people with poor digestion, can cause dizziness through reduced oxygen delivery to the brain and inner ear. Magnesium plays a role in nerve transmission and migraine prevention, and most Americans get less than the recommended intake.
Standard labs often check for these in ranges that are too broad to catch functional deficiency. A vitamin D level of 30 ng/mL may be flagged as "normal" but is well below the level associated with reduced BPPV recurrence in clinical research. B12 in the low 200s pg/mL is technically normal but is associated with neurological symptoms in many patients. Functional medicine uses optimal ranges that match what the research shows is actually protective.
The connection between chronic stress and vertigo is one of the most overlooked but important relationships in vestibular medicine. The vestibular system, the inner ear, and the stress response system are deeply interconnected. Cortisol affects fluid balance in the inner ear, autonomic regulation of blood pressure, and the brain regions that process balance information. When the HPA axis (hypothalamic-pituitary-adrenal axis) becomes dysregulated from chronic stress, it can amplify vestibular symptoms, lengthen recovery times, and lower the threshold for vertigo attacks.
Patients often notice that vertigo episodes cluster around periods of high stress, after big life events, or during seasons of poor sleep. This is not a coincidence, and it is not "all in your head." It reflects a real physiological pattern that DUTCH hormone testing and other functional assessments can quantify. Addressing HPA axis dysfunction usually involves a combination of nutrition, sleep, nervous system regulation practices, and targeted nutrient support.
The last category covers two upstream drivers that few people connect to vertigo. Blood sugar swings, especially reactive hypoglycemia, can cause dizziness and lightheadedness that gets mistaken for vertigo. Insulin resistance and pre-diabetes are also associated with vascular changes that affect the inner ear. For patients with vertigo plus fatigue, brain fog, sugar cravings, or trouble losing weight, a fasting insulin and HbA1c check is worth running.
Gut dysfunction matters because it drives inflammation, and inflammation does not stay in one place. SIBO, dysbiosis, food sensitivities, and leaky gut all contribute to systemic inflammation that can affect the vestibular system. They also impair absorption of the very nutrients (B12, iron, vitamin D, magnesium) that the inner ear depends on. The link between gut health and vertigo is rarely discussed in conventional care, but it is one of the most important threads to pull on for patients whose vertigo does not respond to inner-ear-focused treatment alone.
A functional medicine workup for vertigo starts with what conventional medicine often skips, which is a full review of your history, your lifestyle, and the patterns around your symptoms. When did the episodes start? What changed in your life around that time? What triggers them now? Once that picture is clear, the next step is comprehensive testing to identify the contributing systems. Most patients are surprised by how much information is available when the right tests are ordered and interpreted using optimal ranges.

Testing typically includes a comprehensive blood panel evaluating over 80 biomarkers covering thyroid, blood sugar, vitamin D, B12, iron studies, inflammation markers, and basic metabolic function. For patients with hormonal patterns, DUTCH urine testing gives a detailed picture of cortisol rhythm and sex hormone metabolism. For patients with gut symptoms or suspected food sensitivities, stool analysis (GI-MAP) and food sensitivity testing add another layer. Our advanced lab testing options are selected based on the specific pattern in each case, not a one-size-fits-all panel.
Once the testing identifies the contributing root causes, the care plan addresses each one with specific interventions. That can include nutrition changes, targeted supplementation, stress and nervous system regulation work, sleep optimization, and lifestyle adjustments. There is no template. A patient whose vertigo is primarily driven by hormone shifts and nutrient deficiencies will get a different plan than one whose primary drivers are gut inflammation and blood sugar instability.
Healing the vestibular system rarely happens in a single visit. Follow-up appointments allow the care team to track progress, retest as needed, and adjust protocols based on how the body is responding. Care plans typically run 4 to 7 months, which gives the body enough time to address the underlying drivers and stabilize. Patients usually start noticing changes within the first few months, but full resolution often takes longer because vestibular tissue and nervous system patterns take time to recalibrate.
Understanding the root causes of vertigo starts with the right testing and a care team that takes the time to listen to the full story. Integrative Wellness Centers offers in-person care across Michigan and Zoom consultations for patients in most US states. If you are ready to stop guessing and start getting answers, you can book a consultation with our functional medicine team to begin the conversation.
Realistic expectations matter. Vertigo that has been building for months or years rarely disappears in a single appointment. For patients whose vertigo is driven by BPPV alone, the Epley maneuver plus correcting an underlying vitamin D deficiency may resolve the issue within weeks. For patients with multiple contributing factors (hormones, gut, stress, nutrients), the timeline is usually longer because each thread needs to be unwound in the right order.
Most patients in our practice notice meaningful improvement within the first 6 to 12 weeks of an active care plan, often starting with the easier-to-shift symptoms like brain fog, fatigue, and the intensity of vertigo episodes. Full stabilization, where episodes become rare or stop entirely, often takes the 4 to 7 month timeframe of a complete care plan. Some patients experience temporary flare-ups as the body works through old patterns, which is normal and usually short-lived. The body is designed to be self-healing and self-regulating when the underlying drivers are addressed.
Vertigo is also listed among the symptoms associated with autoimmune conditions, which is why a thorough workup also screens for autoimmune patterns when the history suggests it. Our overview of how autoimmune conditions present walks through the broader symptom picture and the testing approach we use when autoimmunity is suspected.
Most recurrent vertigo gets attributed to BPPV or "inner ear issues," but functional medicine investigates eight root causes that conventional workups often miss, including hormonal shifts, vitamin D and B12 deficiencies, chronic stress, gut dysfunction, and undiagnosed vestibular migraine. The right testing identifies which combination of these is driving vertigo causes in your specific case, which is why patients who plateau on conventional treatment often improve significantly when the full picture is finally assessed.
If you have been searching for answers about vertigo and feel like conventional approaches have not gotten to the root cause, you are not alone. Integrative Wellness Centers works with patients in person across Michigan and via Zoom in most US states to identify what is actually driving these sleep issues. You can schedule a new patient consultation to discuss your specific situation with our care team.
These are the most common questions patients ask about vertigo causes, drawn from real patient conversations and the questions most often searched online. If you have a question that is not addressed here, our team is happy to discuss your specific situation.
1. Can stress and anxiety actually cause vertigo?
Yes. Chronic stress affects the autonomic nervous system and the inner ear's fluid balance, and it can lower the threshold for vestibular symptoms. Anxiety does not invent vertigo, but it can amplify it and make episodes more frequent. Many patients with recurrent vertigo find their episodes cluster around high-stress periods, which is a real physiological pattern, not "all in your head."
2. What is the most common cause of vertigo?
Benign paroxysmal positional vertigo (BPPV) is the most common single cause, accounting for roughly 40 to 50 percent of peripheral vertigo cases. It happens when tiny calcium crystals in the inner ear drift out of position. However, BPPV often has underlying drivers (vitamin D deficiency, hormone shifts, head injury history) that make it more likely to recur if not addressed.
3. Can hormonal changes during perimenopause cause vertigo?
Yes, and this is one of the most underrecognized vertigo causes. Estrogen fluctuations during perimenopause have been linked to new-onset vestibular migraine and increased BPPV risk. Many women develop vertigo for the first time in their 40s or early 50s, and the connection to hormone shifts is rarely raised in standard ENT visits.
4. What vitamin deficiency causes vertigo?
Vitamin D deficiency has the strongest research link to vertigo, especially recurrent BPPV. Vitamin B12 deficiency can cause neurological symptoms including dizziness and balance problems. Iron deficiency contributes to dizziness through reduced oxygen delivery, and magnesium deficiency is linked to migraine and vestibular migraine. Testing all four is worth doing for anyone with chronic vertigo.
5. Why does my vertigo keep coming back?
Recurrent vertigo usually means the underlying driver was not fully addressed. The Epley maneuver fixes the immediate crystal displacement in BPPV, but it does not change why the crystals became dislodged in the first place. Recurrence often points to nutrient deficiencies, hormonal shifts, chronic inflammation, head/neck issues, or a different diagnosis altogether (such as vestibular migraine being misclassified as BPPV).
6. How long does vertigo typically last?
It depends on the cause. BPPV episodes last under a minute and are triggered by head movements. Vestibular migraine episodes can last 5 minutes to 72 hours. Meniere's episodes typically last 20 minutes to several hours. Vestibular neuritis can cause continuous vertigo for several days, with residual unsteadiness lasting weeks. Episodes that last only seconds are often BPPV, while sustained episodes lasting hours point to other causes.
7. Can gut health really affect vertigo?
Yes, though the connection is rarely discussed in conventional care. Gut dysfunction (SIBO, dysbiosis, leaky gut, food sensitivities) drives systemic inflammation and impairs absorption of vitamin D, B12, iron, and magnesium, all of which the vestibular system depends on. Gluten and dairy sensitivities have been linked to Meniere's disease and vestibular migraine in particular. Improving gut health often improves vertigo over time.
If this article resonated with what you have been going through, the next step is finding out whether functional medicine is the right fit for your specific situation. Integrative Wellness Centers has supported thousands of patients since 2012, both in-person across Michigan and via Zoom in most US states. You can request a new patient consultation to start the conversation with our care team and explore what a comprehensive vertigo workup could look like for you.
Medical Disclaimer: This article is for informational and educational purposes only. It is not intended as medical advice and should not replace consultation with a qualified healthcare provider. Integrative Wellness Centers makes no claims to diagnose, treat, cure, or prevent any disease. Always consult your doctor before making changes to your health regimen or discontinuing any medication.

Take the online digestive evaluation to instantly discover what systems of your body are the cause of your health issues.
Online Digestive EvaluationTake the TestOnline Female Hormone EvaluationOnline Male Hormone Evaluation


